
Medications frequently prove ineffective when administered for the mitigation of select conditions. Patients who present with persisting tremors and conditions such as Parkinson’s Disease, epilepsy, and dystonia experience complications with the subthalamic nucleus(STN), globus pallidus internus(GPi), and the ventral intermedius nucleus(VIM) of the thalamus–more generally known as areas within the deep brain. Consequently, deep brain stimulation has become a popular alternative to combatting such complications.
Deep brain stimulation works to provide electrical signals to impact the function of the regions as mentioned earlier. These signals are delivered through carefully implanted leads in the brain whose location is dependent on the area of the deep brain being targeted. Typically, direct high-resolution MRI imaging is done to locate the appropriate physiological structure in need of stimulation. However, the appropriate structure can be indirectly targeted using previously existing stereotactic profiles of the stuctures. Below is a table listing each targeted region with the appropriate positioning of the leads. The leads are placed using framed or frameless stereotactic devices pictured above. Micro-electrode recordings are typically taken before this to ensure the targeted anatomical region is physiologically correct.
Brain Midline Diagram (Jonathan Kitchen Getty Images)
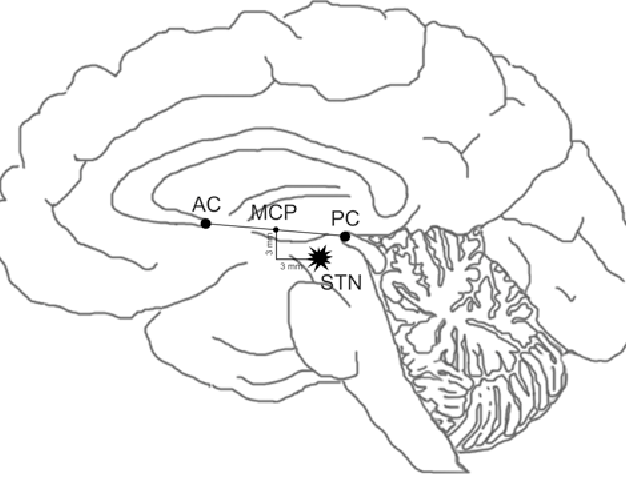
Anterior & Posterior Commissure(AC & PC) with Mid-Commissural Point(MCP) (J Ellen Semantic Scholar)
STN Targeting – Parkinson’s Disease patients
- 11–13 mm to the side of the midline
- 4–5 mm in front of the AC-PC plane
- 3–4 mm behind the MCP
GPi Targeting – Dystonia and Parkinson’s Disease patients
- 19–21 mm to the side of the midline
- 2–3 mm in front of the MCP
- 4–5 mm in front of the AC-PC plane
Thalamus/VIM Targeting – Tremor and epilepsy patients
- 11–12 mm to the side of the wall of the third ventricle(in line with midline)
- At the level of the AC-PC plane
- Between 1/6 – 1/4 of the AC-PC distance in front of the PC

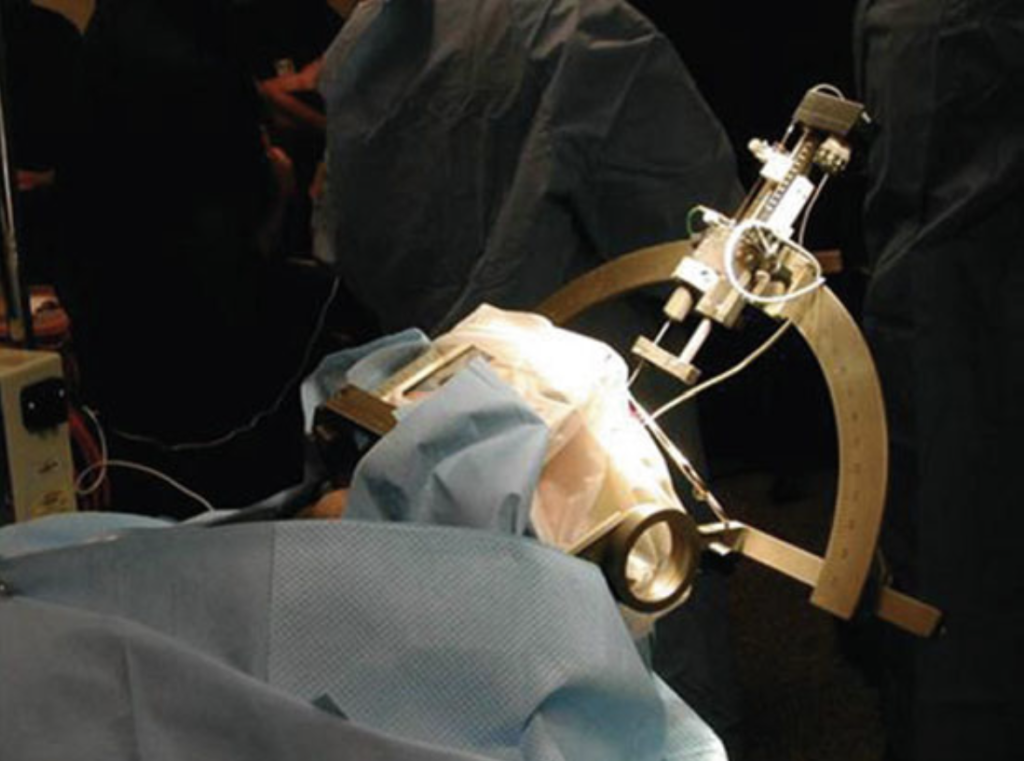
Frameless Apparatus
Apparatus Frame (AR Rezai Surgery for Movement Disorders)
Lead placement can be a very complicated procedure. First, the patient is sedated to allow for one’s head to be placed within a special frame. One’s hair is shaved to allow for easier insertion and the head is secured within the frame with the help of four pins. At this point, the patient’s head can be scanned for the brain’s anatomical regions at which point the patient is increasingly sedated and given anesthetics to allow for the doctor to cut into the scalp. A surgical drill is then used to open into the skull to insert the leads. Depending on the reason for insertion(typically movement disorders), doctors will wake the patient for awake testing. The implantation procedure can be bloody. To confirm there is none and the electrodes are correctly placed, an additional scan is taken.
Once the leads are implanted, they are connected to extension wires which are subsequently connected to an implanted pulse generator within the chest directly under the collarbone. Similar to how a heart pacemaker generates electrical signals to maintain a heartbeat, this battery produces the signals for the leads to deliver to the brain. This is also a surgical procedure involving skin penetration; this is done to create a pouch-like space that will allow for effective insertion. The user is additionally given a controller with which they can turn on or off the signals, allowing the patient to undergo stimulation when they feel necessary.
Deciding whether DBS is the appropriate form of rehabilitation for you can be challenging. It is a rather invasive procedure with a multitude of steps and procedures that must be satisfied for appropriate functioning. DBS is currently only offered to patients who do not see effective results through medications or less invasive means. This can be due to a variety of reasons. Some common reasons include:
- The patient has developed a tolerance towards the medication, requiring a higher dosage to achieve the same effect
- The patient becomes strongly dependent on the medication, requiring multiple doses a day
- The patient is experiencing negative side effects from the medication, including but not limited to nausea, hallucinations, tremors, and dizziness
However, those who do pursue DBS as a rehabilitative measure oftentimes feel relief. Though minor medication use may still be necessary for certain populations, DBS therapy has been responsible for severely limiting, if not halting, medication use. Furthermore, patients are often relieved of their symptoms. Despite the therapy’s invasiveness, it offers a great deal of freedom and control to the patient offering effective results and a stress-free experience. With the consultation of your neurologist, deep brain stimulation may be the rehabilitation you need to see relief from your respective deep brain condition.
Sources:
Deep Brain Stimulation (DBS): What it is, Purpose & procedure. Cleveland Clinic. (2022, May 23). https://my.clevelandclinic.org/health/treatments/21088-deep-brain-stimulation
Deep Brain Stimulation. Johns Hopkins Medicine. (2021, August 8). https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/deep-brain-stimulation
He, B. (2013). Managing Neurological Disorders Using Neuromodulation. In Neural engineering. essay, Springer.
Rezak, M. (n.d.). How does deep brain stimulation work?. Northwestern Medicine. https://www.nm.org/healthbeat/medical-advances/how-does-deep-brain-stimulation-work
